Secre
-
Posts
3078 -
Joined
-
Last visited
-
Days Won
155
Content Type
Profiles
Forums
Events
Everything posted by Secre
-
Jellysundae and Duma are definitely right here. You can only - only - earn np on your main account. You can send np across to side accounts and use it for things like the Neolodge, but it's strict enough that you're not even meant to buy items on your side account. You're meant to buy the item on your main account and send it across to the side account. You can't have a shop, play any games, do any dailies, or in any way earn money on a side account. You can only use them to store pets. You can have galleries on side accounts, but the items need to be bought on your main and transferred. You can enter competitions that have no prizes on your side account, but not competitions like Storytelling etc that have np prizes. You can buy and use NC on your side account, but you can't use cookies on your side. The only exception I believe is the Archive Cookie (because it only gives out NC wearables) and the lab cookie, which you can use on a side ONLY if you don't have the lab ray on your main. You cannot use FQ cookies, lab ray cookies or games cookies on your side. Think of your sides as storage and galleries only and you'll be safe. Yep, it's a big freeze offence!! I wouldn't risk it on a side. If I got a scratch card in a random event on a side, I'd move it over to my main to scratch it. I certainly wouldn't buy scratch cards for use on a side.
-
Squeaked that one at the last minute!! I liked how we all interpreted this differently - I thought everyone would either go Yooyuball or war in honesty!
-
I took the opposite message from last years CC - I spent a fortune on junk to get my points up, so I'm spending an equal fortune but getting over double the loot by prepping in advance this year!!
-
I'm usually fairly useless with sniping, so the last two days have been a definite success! And oh boy do I hate that! Why oh why can they not be removed from the search entirely if frozen!! Yeah, that's what happened. The user confirmed what item it was via neomail and said they couldn't find it on the Shop Wizard so just put a price that seemed expensive on it. I've sent them a combination of a morphing potion, books and collectibles that work out to just shy of a million. I still consider it a good deal mind you, as I got something I was actually looking for for a bunch of things I'd been trying to sell anyway! But they'll likely find the items easier to sell than a petpet paint brush anyway, so I think it's a win win situation!! But yes, particularly as I still remember my long past fail with a transmog potion, I'd have felt far too mean just running off with the snipe. Their account is only a week old!
-
I’m not sure about karma - I did use the item immediately after all!! But I remember making a similar mistake with a Xweetok transmogrification potion as a n00b. Put it into my shop for 99,999np and it went in two seconds flat. I hadn’t realised the Trading Post did bigger ticket sales and that was the shop limit at the time. I still remember it saltily a decade and more later, so I’d hate to do it to someone else. I’m hoping I haven’t been too picky though; I have requested ‘proof’ from the user though; nothing strenuous, just that they confirm the item I bought. I’m wary that whilst I’m relatively confident in my getting back to the right shop, I would likely have snapped the arm off a seasoned user offering me expensive stuff in return for a slight that didn’t actually happen to me as a teenager!! I found it noticeable that they didn’t confirm the paint brush in their initial return neomail... so we shall see. I’ve even given them instructions to Sales Histpry of their shop in case they didn’t know that option existed.
-
So yesterday I found myself a nice 90,000np bargin at 1np. Today, whilst buying fishing junk (I'm obsessed with prepping for CC, I tell you... I have some 19,000 items in my SDB now), I came across a bleeding Mutant Petpet Paint Brush priced at just 50,000np. Current TP asking price? 1.2mil! That's another one of my petpets sorted then - a mutant Ona for my Mutant Draik! *EDIT: I'm feeling guilty having checked the user profile. It's a brand new user. I'm neomailing to confirm it's them I bought from and I'll send a few goodies over to bring the price up to a vaguely reasonable point...
-
I have to admit, if I'd been more on the ball when I bought it, conscience might have overcome me. But by the time I realised what it was worth I was several hundred shops down the line and had no idea who it might be returned to!! So my silly conscience can have no dealings in the matter at all!
-
I randomly picked up a Negg-Gazer Charm for 1np. Thought nothing of it and whacked it in my SDB. Came across another one in a shop for 95,000np. Checked the prices. Gaped for a while. I have no idea who I bought it from, but I'm making some solid profit on that little accidental find!!
-

Favourite neo-achievement of the year? (And neo-resolutions!)
Secre replied to berriganify's topic in Neopets General Chat
In fairness I've just realised that my baby Yurble needs to be taken off that list - that was a this year paint job, although I adopted the pet last year. She's mega cute though: But yes, I'm pleased with the headway I've made on painting pets, particularly as I've kept to my goal of saving neopoints as well! Yeah, I picked up Feed Florg, Korbats Lab, Extreme Herder and Meerca Chase last year - I started on Ummagine, but was nowhere near learning the levels by the end of the year! I'm hoping more games will be released, particularly avatar games. -
Favourite neo-achievement of the year? (And neo-resolutions!)
Secre replied to berriganify's topic in Neopets General Chat
I've been pleased with 2020 on neopets. I've painted a lot of my pets in their dream colours, got quite a few of their petpets and started up a baby and mutant side account. Only the baby account has been really started mind you - I have two babies on it with the eventual aim of at least five plus one lab rat as that's the account I set my lab ray on. Which is another goal done! Pets painted have included HarmBoer becoming his Royal Werelupe cross, FaithfulDarkness becoming a Nightsteed, getting my Mutant Draik via an FFQ and my MSP Poogle via the Premium perk and painting my Peophin Tyrannian on my main. My side accounts have been equally busy with a Darigan Gelert, Woodland Ruki, Plushie Shoyru, Baby Lupe and Baby Yurble. I've also adopted a few well named additions to the family including a Desert Bruce, Clay JubJub and Stealthy Acara Completed petpets include a Tyrannian Feloreena on my Peophin, a Maraquan Snowbunny on my Lutari (who still needs the pet paint job mind you!), a Hegie on my MSP, an Elderly Symol on my first baby pet, a Desert Babaa for my Desert Bruce and a Plushie Doglefox on my Plushie Shoyru. I got into NC trading and have traded for quite a few items for permanent customs and despite buying a ridiculous amount of paint brushes and petpets have still managed to save more neopoints than I had made in my previous seventeen odd years on and off the site! I've also picked up a few avatars as I've been going including some games ones I'd never looked at before. Goals for the New Year include; - a Woodland Rock and Darigan Candychan (that one might be a bit longer coming unless I get lucky at the main shop!) and to organise petpets for my other variety of pets. - Morphing Huggleby into a Halloween Grundo, continuing to collect Baby Pets first but then Mutant pets as well. - Organise my pets onto the correct sides and sort out which pets need painting etc. - Finally getting a lucky zap for that Garlic Kiko. - Continuing to collect avatars although that will be more tricky with the demise of Flash. I got to 248 by the end of 2020, so I'm not sure how many more I'll manage, but at least a handful more I hope. -
Yesterday was an excellent day. Today I think is a day to skip.
-
Yep, mines out too. Pity it's a shared computer or I'd be tempted by the date trick!
-
The Igloo game is glitched and allowing ridiculous scores - a lot of people are having this issue apparently so your cousin doesn't need to worry overly.
-
Current Events: Questions and Answers Over Vaccines and Clinical Trials
Secre replied to Secre's topic in The Debate Chat
I'm perfectly fine with you sharing to Facebook - there's a share button in the .... section at the top of the post I've just found! I suspect I've got quite a wait before I'm notified it's my turn as I'm not in any of the high risk categories - my work in clinical research isn't patient facing, so I don't count as frontline staff. Yep, I get a lot of people just refusing to listen. I've almost given up trying to persuade the real detractors, but hope that by putting key information alongside their theories, others might be able to get the facts rather than believing what they see on Facebook. Well, that's better than the alternative of not taking it at all! Not good for the surgery mind you!! I know several places got their vaccine doses last Friday, so hopefully things will get rolling. But as I mentioned above, I still don't think most of us will get them until March-April unless we're in the high risk groups!! My grandmother (in law) got her first doses already and she's in her 90's. My grandfather (in law) is waiting on further research data about contra-indications with warfarin I believe though! -
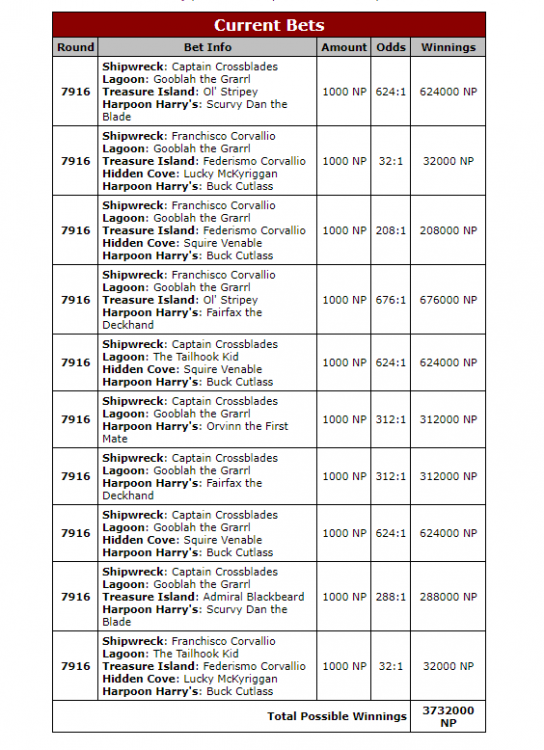
I've done slightly better than Garet these last two days; 16:10 instead of 12:10 and 20;10 instead of 16:10. I've gone with Garet today again, but taken out the Orvinn safety and added in a 4 pirate base bet at 16:10, so if the 2:1's come in I make quite a lot more.
-
Current Events: Questions and Answers Over Vaccines and Clinical Trials
Secre replied to Secre's topic in The Debate Chat
Thanks! It ended up being a little longer than I had planned, I must admit but I figured the extra information might be useful to someone at least. I think if I had a choice, I would want the Pfizer or the Moderna vaccine as they have the best efficiency figures. I suspect we won't get a choice, it will just be whatever the local NHS Trusts have managed to get a supply of. The Oxford vaccine still have a good efficiency percentage though, just not quite as good as the other two. I think part of the issue we're having with people refusing to contemplate having the vaccine is down to just how niche an understanding of how clinical research actually works is. If you don't work directly in the sector, it is expected that you will just trust the experts and in today's world, people don't trust the experts not to lie to them. I'm hoping that by explaining some of the nuances of the trial systems - not just here, but on a variety of public sources - I can improve understanding and hopefully reduce some of the fears people have about the vaccines. I live in hope! -
Nope, apparently 2:1's all won, but not the ones that I deemed most likely. I knew that was the likely option when I chose to do a daft bets day in the face of the appalling odds though!! I've followed Boochi to the letter today.
-
I seem to spend a lot of time scouring Facebook and addressing concerns and fears over the latest coronavirus vaccines. So I thought I'd open a topic to see if there are any concerns here. Mods - I believe this would be permissible by forum rules, as we don't have the same strict 'no current events' rules that neopets have. If I have misinterpreted this, please feel free to remove. As some background, I have worked in clinical trials for a number of years (eight to my current reckoning, or at least there about) and know a reasonable amount about the background of trials. I do not directly work in coronavirus trials, although my unit has run three trials in the area within the last twelve months. I specialise in cancer trials and have worked on three large scale trials involving IMP's (investigational medications) across prostate cancer, small cell lung cancer and currently neuroblastoma in children. I did a brief stint in muscularskeletal trials where I largely supported non-IMP trials, which are trials that do not use any investigational medications and have also supported data collection in sample trials. The scientific rationale behind vaccines themselves is not my area of expertise, although I have a decent understanding. I do have contacts within the scientific community I can approach if anyone has any specific scientific queries I cannot answer. I'll start with some common concerns I have heard and can address from a trials perspective. Has The Vaccine Been Made Too Quickly To Be Safe? The short answer is no. The three drugs that are currently licensed as vaccines in the UK have all gone through Phase I, Phase II and Phase III trials, with robust and strict safety procedures. The long answer is still no, but comes with some more detailed information on how trials usually work. In the UK, we have to jump through a lot of hoops and a lot of red tape to even get a trial open for recruitment. The average time it takes for us to get a trial open to recruitment is between two and three years. This is because protocols and statistical analysis plans need to be drawn, we have to apply for and receive funding before we can even start looking for approvals, we need to apply for regulatory and ethical approvals, we need to canvas potential sites and get them interested before then setting them up, we need to set up contracts for each individual site and get data collection tools in place. This is an excellent guide to just how much goes on behind the scenes before we can get a trial recruiting: https://www.ct-toolkit.ac.uk/routemap/ In contrast, my unit has run three COVID-19 trials in the last twelve months - CATALYST, PACE and COVID19 BMT. Two of them were set up and recruiting in six weeks, one took slightly longer at seven weeks. This is unprecedented, but it is not unsafe. Why? Because the red tape was cut. COVID-19 has sparked such a wave of scientific, political and public interest that funding was being thrown around. approvals were being fast tracked and sites were clamouring to be included. Things that would normally involve months of waiting. took weeks or even days. Things moved quickly, but that doesn't mean the protocols or development plans were less robust; it means we cut out the waiting times. Once we get a trial up and running, it can often take years to recruit enough patients to analyse the data. This is because we are often dealing with rare diseases or small sub-groups of patients. The BEACON trial is in relapsed/refractory neuroblastoma patients - neuroblastoma in children is rare to begin with, but the patients we are looking to recruit are advanced disease patients and that makes our sub-group even smaller and so it has taken us five years to reach 220 patients with over thirty sites involved. This is the same across many trials. We often have to recruit internationally to have a chance of hitting the recruitment targets. In contrast. two of the studies I referenced have completed recruitment and are in analysis and the final one is nearing the end of recruitment. There are hundreds of thousands of potential patients as opposed to the handful we get in smaller trials. For the CATALYST trial there are only six sites involved and all are in the UK. There is no need to spend all the extra time opening international sites, because the target population is large enough to be done even with a small number of sites in the UK. Getting the patients more quickly means getting the data more quickly. It means follow up points can be hit in a fraction of the time as the patients are all in and receiving treatment. So in essence. speed does not mean a lack of testing or a decrease in safety. If anything. the speed these trials have been opened and recruited is a testament to how smooth clinical research could be in the future. How Can They Know What The Side Effects Are? The short answer is that every trial involve a thorough Adverse Event Reporting Procedure to be in place before any drug is licensed. This is no different in COVID-19 vaccine trials. We are legally (and morally) required to collect data on potential side effects in any trial. The scienctific term for this is pharmacoviligence and it is taken exceptionally seriously within clinical trials. The long answer once again comes with some more detailed information on how trials usually work. Every trial comes with an entire collection of Case Report Forms (CRF's) that are entered into large databases; these include: - Pre-trial data such as pre-existing conditions and screening criteria. For cancer trials we also collect specific data such as tumour measurements and assessments to be assessed against later forms. - Trial data such as pre-treatment forms documenting the assessments done before each treatment, treatment forms documenting what trial drugs the patient was given, con-medication forms documenting what non-trial drugs the patient received at the same time and adverse event forms collecting every single sniffle, whiffy blood test and scrape and bruise. For cancer trials we also continue to collect tumour assessements for obvious reasons. - Follow up data which are collected at set points defined by the trial protocol. We usually collect Adverse Events for 28 days following last treatment and then collect more basic data at set points. This may be every three months, six months etc depending on the protocol. The Adverse Event Forms are the most crucial to this question though. Throughout any trial, we are legally mandated to collect data on every adverse event a patient may experience during the trial. This is not just side effects, this is every single event. So if a patient falls over and breaks their wrist, that has to be reported. If a patient gets a cold or a lung infection, that has to be reported. The full list of everything is here and it is pretty exhaustive even without the 'Other' category for anything that might fall through the cracks: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf. Throughout the course of a single trial, there will be hundreds if not thousands of AE's reported. Some of these will have no relevance to the trial; so if a kid falls over and breaks their wrist, that won't be flagged. But if ten kids fell and broke their wrists, this would be flagged for assessment as a potential concern for bone weakening with the drug. Some side effects are expected. others are not and it all comes down to what is shown by the analysis of the overall data. All of this data is analysed throughout and at the end of each trial. It is presented to a specific committee made up of consultants and experts in the field that looks at the unblinded data (so can see which side effects are only on trial IMP arms of the study) and makes a decision as to whether it is safe to continue. In addition to this basic level of reporting, there is also a process called Serious Adverse Event/Reaction (SAE/R) reporting in trials. An SAE is any adverse event that causes hospitalisation, prolonged hospitalisation, is life-threatening, causes congenital/birth abnormalities or results in death. And these are taken incredibly seriously. Additionally, any SAE is also reported as a regular AE to ensure it is included in the main analysis data. There are strict time frames associated with how quickly we have to report these more severe events to our reporting agency and all of these events are individually assessed by the site consultant and then by the lead investigating consultant on the trial. One of the assessments is whether the event is linked to the drug - if it's not, like that random kid who decided to fall out of a tree referenced earlier, then it is an SAE and we go about our business as normal. If it's could in any way be linked to the treatment, then it is escalated to an SAR (reaction rather than event) and then a second level of assessment is done. At this point it is determined if it is an expected side effect and this is where all hell can break loose. Because if we get an event that is not anticipated then this becomes a SUSAR - our acronyms become silly here and it stands for Suspected Unexpected Serious Adverse Reaction. The reporting time frames become even stricter and this is the kind of event that stops trials. If we don't have enough data, we have to assume the worst - which is why the Janssen and Oxford vaccine trials were both paused. Once more data comes in, the event can then be re-classified if it is not considered linked to the drug. What is important to note is that most trials do not collect adverse event data after a certain period - so in cancer trials this is typically 28 days. If there are any suspected SUSAR's however, these can be reported years after the trial has finished. What happens at this point is that the drug is (hopefully) licensed and the post-licensing period is known as the Phase IV trial. The drug is being prescribed and we rely on doctors to report any unexpected side effects via the Yellow Card scheme - https://yellowcard.mhra.gov.uk/the-yellow-card-scheme/. This is standard procedure for all new drugs. it is important to note that actually the COVID-19 trials are more likely to have noticed any rare adverse events. This is down to the simple numbers game. Our Phase III trials recruit anywhere between 250 and 400 patients as standard; if there's a rare event that might be seen in 1 in 1000 patients, there is a high chance we will not find it. It will come out after the drug has been licensed, in the Phase IV stage. In contrast, the COVID-19 trials have recruited tens of thousands of patients. These are some of the largest and most comprehensive trials in the UK in modern history. The Phase III Oxford vaccine trial alone involved 11,636 volunteers, the Pfizer trial randomised 43,548 patients. They have enough patients to be pretty certain about the side effects. The Success Rate of the Vaccine is lower than the Survival Rate of the Disease, Is It Worth It? The short answer? Yes. If we can stop 90% of the population from even catching it, we will stop the spread of infection in its tracks. We will protect our families, who may be at higher risk than ourselves and we will protect ourselves from long term complications. The long answer. Let's take this one in parts. First of all, the question doesn't really make sense. Even if the vaccine was only 50% effective, it would still be worthwhile. At 50% efficacy, that would half transmission rates and bring that dreaded R number all the way down. At the actual success rates which seem to be within 80-95% depending on the drug (the Pfizer drug trials show 95% efficacy, the Oxford drug trials show 70-90% efficacy depending on how the drug was administered), this would be a huge boon to decreasing infection rates in the population. That will in turn protect the highest risk members of the community; if there are less cases in the community, there is significantly less chance that grandma will catch it. Secondly, whilst COVID-19 has an average survival rate of 98-99%, survival doesn't equate to complete recovery. Survival means exactly that, it means you didn't die. Death is not the only concern though, and there are significant long-term complications present even in patients who were in low risk groups. These include those left with long-term respiratory or cardiovascular damage, inflammatory disorders, and clotting disorders. We do not yet know how badly those effects will affect life expectancy and quality of life. Other long-term effects that may have a significant impact on health and well-being involve mental health, gastrointestinal effects and possibly neurological effects. SARS is not the same disease, so any comparison has to be taken with a grain of salt, however there are many similarities and we know that there is a persistent and significant impairment of health status in survivors of SARS over 24 months - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7192220/ and that a significant percentage of survivors still had chronic fatigue symptoms 3.5 years after being diagnosed - https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/415378. Essentially, it is important that you do not confuse ‘survival data’ with complete recovery. You have an excellent chance of surviving COVID-19 if you are not in an at-risk group, but the chances of also having long term medical implications after the fact are also high. Will The Vaccine Change My DNA? Can I Catch COVID From The Vaccine? Short answer; no and no. mRNA vaccines are new and hugely exciting as they are ground-breaking research, but do not change your DNA. None of the licensed vaccines include live viral particles, so you cannot catch COVID-19 from any of them. The long answer is a little more out of my comfort zone in terms of the high science end, but can be explained fairly basically. - The Oxford vaccine is a chimpanzee adenovirus vaccine vector which causes the common cold in chimpanzees. It does include a live virus, but it does not include live coronavirus. Essentially they modify the live adenovirus so it is unable to cause the disease in humans, then take the spike protein from the coronavirus and genetically sequence it into the vaccine vector. When this is injected, it primes the body's immune system to recognise and attack coronavirus if you are infected. - Both the Pfizer and the Moderna vaccines are mRNA vaccines, which have caused more of the concern on the DNA front. They contain material from the virus that causes COVID-19 that gives our cells instructions for how to make a harmless protein that is unique to the virus. After our cells make copies of the protein, they destroy the genetic material from the vaccine. This protein then primes the body's immune system to recognise and attack coronavirus if you are infected. So this vaccine does not alter your DNA or cause you to contract COVID-19. It is also worth noting that whilst these RNA vaccines are the first to be approved for use in diseases, it is not new technology. Scientists and researchers have been RNA technology for a while and there are clinical trials using them in various cancer types. Hopefully that has been of some use. I'm happy to answer questions where I can and to ask contacts for further information where my knowledge is lacking.
-
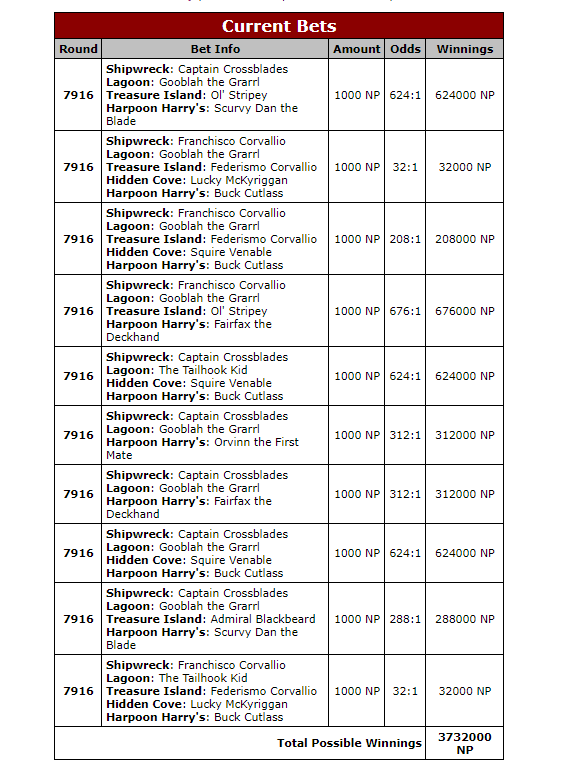
Today's odds are appalling. So as it's undeniably a Skip Day, I have thrown 1000np per bet and gone YOLO. I will almost certainly lose 10,000np but if I come up trumps, I'll come up trumps with an extortionate amount for my buck. There is no rhyme or reason to these bets, other than finding the highest odds and running with them. I do not expect to win!!
-
I actually really like both sets of clothing. The Steampunk helmet is a tad overdone for my liking, particularly considering how streamlined the torso of the outfit is. But that torso would work nicely with several other colours which is good for cross-painting. I'm not keen on the bland beigeness of the base colour. It's a bit meh. I far prefer the darker base that is used on several of the pets. I think the outfit looks far superior on one of the darker base colours: The outfit is adorable though! Honestly almost makes me want to go get an Aisha!!! I love the ears and the ruffed cloak. The cloak looks more royal than the actual Royal Girl items!





-
Whilst the outfit is a tad busy I actually like it - it makes me think of a plushie somehow. I think I prefer my woodland colours a bit darker though. It's nicely designed, but not my cuppa tea.
-
Yeah... the relic is... not good. The base is good... but I think it's meant to be moss but looks like snot!? What happened!? I always think the base should be a removable clothing item as well as it gets in the way of customs. The space themed clothing is good though!
-
Possibly. I got one score sent but my other four attempts were less successful. Thankfully it's a short enough 'game' that you don't care so much!
-
I'd add that the really low selection of games - and how buggy most of them seem to be - is a shame. I can't actually get a score to send on Fashion Fever as it says Invalid Session, Turmac Roll is laggy and doesn't register all of the berries and the screen for Ice Cream Machine seems smaller (not sure if that's my imagination) and again there's a lag as the ice creams fall which makes the game frustrating. I'm not sure I have the heart to try out the few remaining games that have been converted until they iron out the kinks rather more.
-
I'll have a go at putting something together then - having taken a break over Christmas, I didn't have enough time to cobble two outfits together yesterday, but with an extra week we should be good!!